Chapter contents
I. Introduction
Medications and lifestyle changes can help HS in a lot of ways, but oftentimes HS is not completely controlled by medications. In these cases, surgery can be helpful for treating stubborn tunnels and scars. Surgery is most often recommended as a treatment option for lesions that have been present for months or years; surgery is usually not initially suggested for newly formed lesions that are likely to heal on their own. Surgery can also be an option for people that dislike medications or have had unpleasant side effects from them in the past. However, the risk of recurrence and need for more surgery may be higher when medications are not also included in the treatment plan to manage your HS.
II. Types of Surgery
There are two main types of surgery for HS: deroofing and excisions.
Deroofing
Deroofing (or unroofing) is when the healthcare provider removes all or most of the skin overlying a tunnel or pocket to expose the inside and remove pus or inflamed skin.
This leaves a shallow wound that does not penetrate the full thickness of the skin. This procedure can be done in a clinic using local anesthesia where you are injected with numbing medicine, but may also be performed in an operating room using general anesthesia where you are put to sleep for the surgery.
Once the area is numb, the healthcare provider will use a scalpel, scissors, or other surgical tools to remove the top of the lesion and clean out any inflamed material. Your dermatologist may use a scraping tool called a curette to remove some of the material in the tunnel. A small metal rod may be used to probe the area and make sure no tunnels remain. The deroofing site will usually be left to heal on its own, as stitches can trap diseased skin or other debris under the surface and lead to the formation of more tunnels or pockets (Figure 21.1).
Excision.
The other main HS surgical technique is excision, which involves removing the entire lesion including the underlying skin layer.
Excisions can be performed on single lesions or on body sites, such as an armpit. Just like the deroofing procedure, an excision can be performed in a clinic with numbing medicine or in

• Figure 1: Deroofing procedure: A. After numbing the skin a metal rod (probe) is used to explore the tunnel, B. The surgeon uses scissors to remove the top of the lesion, “deroofing” the sinus tract, C. Immediately after deroofing the wound is left open to heal, D. 12 weeks after deroofing the wound is healed.
the operating room while under anesthesia. Because excisions are deeper, the resulting wound may be larger. Unlike deroofings, excisions do not leave part of the tunnel at the bottom of the wound so it may be possible for an excision wound to be stitched up (Figure 21.2).
The decision to stitch the wound may depend on factors like size and location. Larger wounds are harder to pull together, and may lead to stitched wounds that feel tight and restrictive. It is unclear if stitching excision wounds increases risk of recurrence compared to letting the wound heal by itself, and some doctors prefer to avoid it. In some cases, surgical repair of excisions can be performed with skin grafts taken from another part of your body. Your healthcare provider may also choose to use a “flap” which rotates and/or pulls skin from beside the surgery site to cover the wound. This can allow a large wound to be closed, but may result in a bigger surgical wound and longer recovery. Excisions are also discussed in Chapter 22.
III. Recovery After Surgery
For most people with HS, the pain is worst in the first three to five days following surgery, though many people feel the surgical pain is not much worse than a bad HS flare. You may require extra pain medication and time to recover on those days. Pain is typically managed well with over-the counter medications like acetaminophen/paracetamol (Tylenol®) or non-steroidal anti-inflammatories like ibuprofen (e.g., Advil®). For smaller procedures, most people can return to work in a few days. With larger procedures, it may require a few weeks to recover. Most wounds heal over three to six weeks as the edges pull together to form a scar. While recovery has its challenges, most people with HS have experience with wound care and feel like they can handle it well.
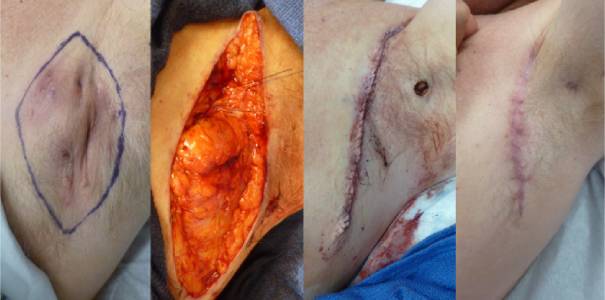
• Figure 2: Excision of HS: A. The surgical site is outlined, B. The skin has been excised down to the fat layer, C. The wound is stitched together, D. 12 weeks after surgery the wound is healed in a curved scar
IV. Post-Operative Care
It is important to keep the wound covered and protected after surgery. It may be helpful to wear loose clothing for the first few days so that your clothes do not rub the area. Once the scar has formed, your doctor may have you perform stretches to ensure that the wound heals properly and does not restrict movement. The pain, swelling, and typical wound discharge should gradually improve each day. If it worsens, you should let a healthcare provider know in case there is an infection that requires attention. A small amount of bleeding on the bandage may also occur, but you should notify your healthcare provider if the wound bleeds through the bandage.
For deroofing procedures, wounds typically only need petroleum jelly (e.g., Vaseline®) and a nonstick dressing applied directly, but doctors may have different suggestions for wound care. Dressings should typically be changed at least daily after gentle cleansing, as suggested by your doctor.
For very large wounds, it is possible that your doctor will use a special vacuum-assisted closure (VAC) technique, which seals a small suction tube in the wound under a sticky seal. This or other drain types may require additional care. In some instances, a second surgery is planned following the first procedure to close a wound, once it has healed to a smaller size.
V. Surgery Benefits
One of the greatest benefits of surgery is that it can remove stubborn tunnels and scars that respond incompletely to medication.
Since HS is a disease that can fluctuate between periods of activity and inactivity, it is possible for HS to come back at or nearby the surgery area. Risk of recurrence can depend on several factors, including the severity of your disease, how many locations are affected, how long you have had HS, where your lesions are located, and what kind of surgery is performed. Factors that increase the risk of recurrence include younger age, more affected areas, more severe disease, and surgery in the genital area. However, many people with HS with these traits still have excellent results.
Varying rates of recurrence have been reported following surgery, which may be influenced by the factors above. With deroofing, reported rates of recurrence ranged from 14-27%. With excisions, recurrence rates were reported between 13-33%. This means that, with either surgery, there is around a 70-85% chance that lesions will not return in the area that was operated on. If you do get more lesions, it does not mean that the surgery has failed. Part of the nature of HS is that it does tend to recur, but recurrences after surgery are typically not as severe.
Given the high rates of success, most people with HS are pleased with their surgical results. 90% of people with HS who underwent deroofing procedures would recommend the procedure to others. Similarly, 92% of people with HS who had a wide excision would recommend it to others, and 50% reported that the surgery had a medium to major positive impact on their lives.
VI. Conclusion
Ultimately, it is important to remember that surgery is a shared decision between you and your doctors.
You should voice your goals and concerns so that you feel comfortable with the timing and size of the procedures, though sometimes decisions may be influenced by what procedures your surgeon has experience with. Not all dermatologists are familiar with surgery for HS, so a referral might be needed.
It is important to remember that surgery is just one part of managing HS. Especially in severe cases, medication can be key to helping reduce inflammation and prevent surgical complications, allowing for better wound healing.
VII. Questions and Answers
Question 1 My regular healthcare provider does not perform these surgeries. What kind of healthcare provider typically performs surgeries? How can I find a surgeon that can help me? AnswerSome dermatologists can perform these surgeries, but some do not feel comfortable with it. Thus, it may be helpful to find a surgeon that specializes in HS. You can find a list of HS specialty clinics on support websites like HS Foundation (https://www.hs-foundation.org/hs-specialty-clinics). you can also ask your main HS healthcare provider if they have any recommendations. Sometimes social media and online support groups can be helpful in identifying local surgeons, though we recommend using these resources with caution. For larger surgical procedures, and when people prefer to be under general anesthesia (fully asleep), it is more likely that a general surgeon or plastic surgeon would perform the procedure. Furthermore, specialized surgeons may be involved in surgeries performed on certain locations on the body, such as a urologist for the groin or colorectal surgeon for areas near the anus.
Question 2 Who is a good candidate for surgery? What could make me a bad surgical candidate or prevent me from getting surgery? AnswerSurgery is typically best for people who have not achieved good control of their disease through medication alone. Their lesions have typically been present for months or years, such as tunnels or sinus tracts that repeatedly become inflamed.
Some surgeons may feel uncomfortable operating on people with HS who smoke, have poorly controlled diabetes, or are very overweight. While studies have not clearly shown that these factors create major problems with healing for HS patients post-surgery, many surgeons are concerned that these factors could complicate wound healing. Certain conditions might also increase the risk of complications relating to general anesthesia.
Question 3 Is there anything that I can do before surgery to improve my outcome? AnswerGood control of inflammation related to HS can help make HS surgical procedures easier and help healing go more smoothly. Skin that is very inflamed may heal more slowly. Using medications when needed to control your HS before surgery and during healing is usually helpful.
If you want to ensure the best recovery, stopping smoking may be helpful. There are numerous ways to help you quit smoking — just ask your healthcare provider. Most studies of surgery for HS included many patients that smoked, and the majority of those patients still benefited. Quitting smoking may be helpful, but surgery can still be beneficial when quitting has been hard.
Having good control of your diabetes can also help to ensure that your wounds heal properly. Your primary healthcare provider can do a quick blood test to check how well your diabetes is managed, and they can work with you to adjust your medications as needed. Patients with diabetes can still heal well from surgery, but improving control of diabetes may help speed the healing process after surgery for HS.
Question 4 If surgery works well, why not just get all areas affected by HS surgically removed as a cure? AnswerSometimes surgery alone can be very effective. This is most often the case for people with HS that rarely develop new lesions and just have a few stubborn areas with tunnels that keep getting inflamed. In a case like this, surgery alone could be considered.
For many people with HS, however, there is a mix of old and new lesions, and removing old ones will not necessarily keep new ones from forming. Thus, it is usually best to stabilize HS with medicines first, then pursue surgery for areas that do not completely improve. Some people with HS who do not have good control of new flares end up having many procedures over time as new areas continue to pop up.
Question 5 Will I need to stop my medications before or after the surgery? AnswerMost people with HS can continue their medications without interruption, but it is important to review all your medications with your healthcare provider before undergoing surgery. Some medications used to treat HS may suppress your ability to fight infection, which can be important following surgery. However, having your disease well-controlled can reduce the risk of surgical complications. Notably, the “SHARPS” study found that adalimumab (Humira®) does not impact healing and can be continued during surgery. Your provider will consider these factors and help you to make a plan that is best for your situation.